NPH phenotypically presents either as isolated renal disease or as a complex syndrome with manifestation in multiple organs. Most often affected organs are the eyes, liver, skeleton or the central nervous system:
Ophthalmological phenotype:
The eyes are most frequently affected in NPH. A rough distinction in two different ways of affection is made: the impairment of ocular movements (oculomotor apraxia e.g. Cogan) and disorders of the retina (retinitis pigmentosa e.g. Senior – Løken Syndrome). The severe congenital form of retinitis pigmentosa (Leber’s congenital amaurosis) is associated with congenital blindness, nystagmus and pupils unresponsive to light. Retinitis pigmentosa has a later onset, first manifests with night blindness and has a slow progress of visual impairment.
Central nervous system:
Different neurological abnormalities can be associated with NPH including oculomotor apraxia, cerebellar hypoplasia, muscular hypotension, seizures, encephalocele, delay of speech development and cognitive impairment.
Skeleton:
Polydactyly, short finger and thoracic deformation are for instance common in Jeune asphyxiating thoracic dysplasia. Cone shaped epiphysis are characteristic for Mainzer – Saldino syndrome. Different other skeletal abnormalities can be associated with NPH and are summarized as ciliary chondrodysplasic syndromes.
Liver:
Congenital liver fibrosis can be found in different ciliopathies (e.g. Boichis syndrome, Arima syndrome, Meckel – Gruber syndrome) and can be isolated or associated with NPH and abnormalities in other organs.
Situs inversus and congenital heart defects:
Situs inversus and congenital heart defects (especially atrial septal defect) are most common in infantile NPH but can also be found in other ciliopathies.
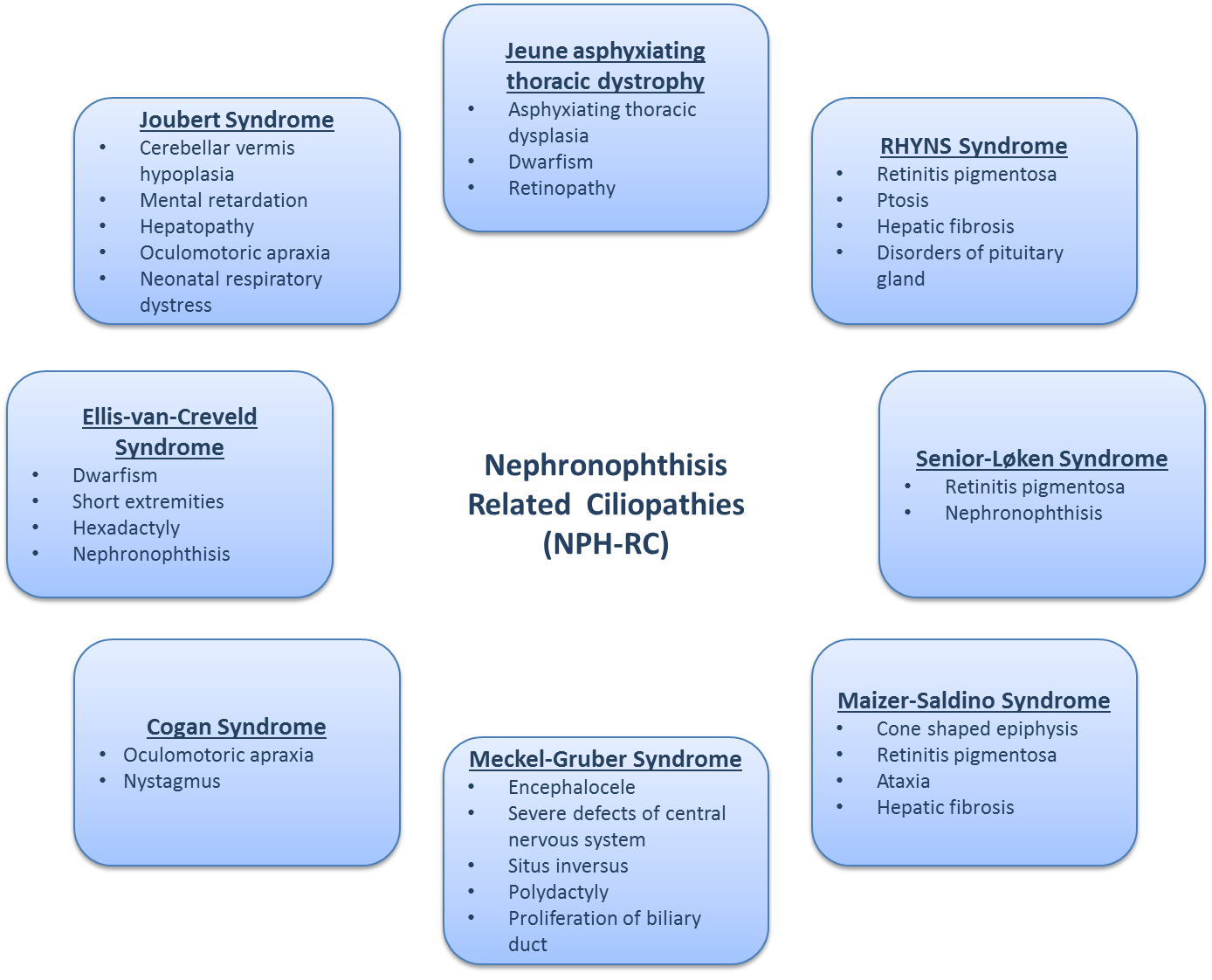
NPH can appear as a renal manifestation of clearly defined syndromes summarized as NPH related ciliopathies (NPH – RC). The following picture shows the most important syndromes:
| Eyes | retinitis pigmentosa | Senior-Løken syndrome |
| Bardet-Biedl syndrome | ||
| Arima syndrome (cerebro-oculo-hepato-renal syndrome) | ||
| Alstrom syndrome | ||
| RHYNS syndrome | ||
| oculomotor apraxia | Cogan syndrome | |
| nystagmus | Joubert syndrome and associated disease | |
| coloboma | COACH syndrome | |
| CNS | encephalocele | Meckel – Gruber syndrome |
| aplasia of the vermis | Joubert syndrome and associated diseases | |
| hypopituitarism | RHYNS syndrome | |
| Liver | hepatic fibrosis | Boichis syndrome |
| Meckel – Gruber syndrome | ||
| Arima syndrome | ||
| Joubert syndrome and associated diseases | ||
| Skeleton | short ribs | Jeune asphyxiatign thoracic dysplasia |
| cone shaped epiphyses | Mainzer – Saldino syndrome | |
| polydaktyly | Joubert syndrome and associated diseases | |
| Bardet – Biedl syndrome | ||
| Ellis-van-Creveld syndrome | ||
| other skeletal abnormalities | Cranioectodermale dysplasia/ Sensenbrenner syndrome | |
| Ellis-van-Creveld syndrome | ||
| other defects: situs inversus, congenital heart defect | ||
sources
- Wolf M. Nephronophthisis and related syndromes. Curr Opin Pediatr. 2015 Apr; 27(2): 201–211.
- Huber C, Cormier-Daire V. Ciliary disorder of the skeleton. Am J Med Genet C Semin Med Genet. 2012;160C:165–74.
- Otto EA, Schermer B, Obara T, et al. Mutations in INVS encoding inversin cause nephronophthisis type 2, linking renal cystic disease to the function of primary cilia and left-right axis determination. Nat Genet. 2003;34:413–420.